

KNEE CARTILAGE INJURIES AND ARTHRITIS
Knee Cartilage Injuries and Arthritis
Arthritis is a condition in which one or more joints (prefix: arth-) are inflamed (suffix: -itis). Virtually any joint in the body can become inflamed, but arthritis in the knee is very common. Knee arthritis can be very painful and even disabling.
People with knee arthritis may have trouble with even the simplest of tasks basic mobility, like walking or climbing stairs. Knee arthritis usually occurs in older people, but it can sometimes develop in children as well. Fortunately, several effective knee arthritis treatments are available from your knee arthritis doctor in New York City.
Hyaline Cartilage
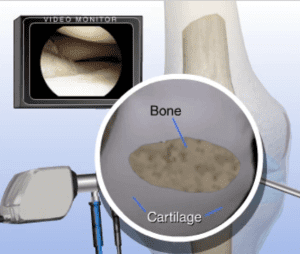
Hyaline cartilage is the specialized material that covers the articulating surfaces of the knee. It is less then 10mm in thickness and has a white/bluish glistening appearance. Hyaline cartilage functions to provide a low friction surface with elastic properties the sum of which allows for smooth motion in the joint with the ability to absorb mechanical stress so that it is not transferred to the bone. The way it does this is by having a very smooth low friction surface and by being able to compress (lose height) and then spring back (normal height) when the applied stress is removed.
The Hyaline Cartilage material is composed of primarily collagen type 2 which provides the structure to the material; in addition there are proteoglycans . Proteoglycans consist of a core protein with an attached glycasominoglycan (GAG). The GAGs are carbohydrates such as chondroitin sulfate and are negatively charged (anion) and as a result have a propensity to bind positively charged ions such as water, sodium, calcium, potassium (cation)). The combination of the collagen and proteoglycans make up the extracellular matrix of the hyaline cartilage which is responsive for the material(mechanical ) properties. This matrix is generated (produced) by the resident cells which is dispersed within the material in spaces called lacunae the cells themselves being called chondrocytes (these are the workers that maintain the house by constantly repairing and replacing damaged parts). Cartilage is devoid of blood circulation and nerve endings.
Hyaline Cartilage Physiology
Hyaline cartilage is devoid of a blood supply and derives its nutrition from the synovial fluid. The material properties of the hyaline cartilage are made possible by the ability of the hyaline cartilage to work with synovial fluid to create an extremely low friction surface (see synovial fluid). In addition, the hyaline cartilage has the ability to absorb stress based on its elastic properties made possible by its ability to compress and then spring back. This happens largely from the release and then reabsorption of water from the extracellular matrix. In order for the hyaline cartilage to remain healthy, the chondrocytes need to be functioning properly for constantly repairing the extracellular matrix. There also needs to be sufficient substrate (building blocks) to perform these repairs (protein, calcium, potassium, chondroitin sulfate etc). The synovial fluid needs to be present and have the proper material properties being produced and maintained by the synoviocytes which also need the proper substrate (building blocks) to create the product (ie. hyaluronic acid).
Synovial Fluid Anatomy and Physiology
Synovial fluid is a viscous material that bathes the joint surfaces; composed of hyaluronic acid (composed of glucuronic acid and glucosamine), lubricin (boundary level lubrication) , proteinases and collagenases. It is produced by cells in the synovial membrane- synoviocytes.
It reduces the friction of the articulating joint surfaces and also has the rare property of becoming more viscous as the magnitude of the applied load increases (non-Newtonian Flow) as well as being thixotropic – the fluid thins and viscosity decreases over a period of continued stress. These material properties both function to protect the surface of the joint..
Synovial fluid is also responsible for delivering oxygen and nutrients to the chondrocytes (hyaline cartilage) as well as removing C02 and metabolic waste from the joint.
Hyaline Cartilage Injury and Symptoms
The symptoms of hyaline cartilage injury can be a gradual onset in the setting of arthritis or can be more acute in the context of a traumatic event. Pain, difficulty with weight bearing, weakness, limping, swelling, locking episodes, inability to perform sports, or run or jump painlessly can all be symptoms of injury. Knee arthritis is the general term applied to almost all forms of hyaline cartilage injury/damage and is separated into two broad categories- Non-Inflammatory and Inflammatory.
Types of Arthritis That Affect the Knee
There are many different kinds of knee arthritis, but the three most common are osteoarthritis, rheumatoid arthritis, and posttraumatic arthritis. Knee cartilage injuries and arthritis are closely related. For example, a small knee cartilage injury can lead to osteoarthritis or posttraumatic arthritis.
On the other hand, if rheumatoid arthritis of the knee is left untreated, it can cause severe structural damage to the knee. Since knee arthritis treatments are different depending on the type of arthritis, it is important to know which type of arthritis you have.
Non-Inflammatory Knee Arthritis (Cartilage Injury)
The hyaline cartilage surfaces can be damaged as a result of repetitive stress and time. This is a degenerative process of cartilage change and is called osteoarthritis. This is the common type of cartilage damage that is experienced by many people.
Damage to the cartilage surface in this category generally occurs along a spectrum of change beginning with softening of the cartilage which then progresses to superficial cracking and then deeper cracks followed by erosions and eventually areas of complete cartilage loss. These spectrums of changes are referred to as chondromalacia.
The cartilage surface can also be damaged as a result of a single traumatic event. This can happen with a dislocation episode such as that encountered in an ACL injury or a patella dislocation. It can also happen with a knee fracture of the bone, which extends into the joint disrupting the joint surface.
This type of damage is often referred to as a traumatic defect distinguished often by its focal geography and can often be measured in very discrete terms with surrounding healthy cartilage. This appearance could be altered obviously, if the joint was degenerating prior to the traumatic event having occurred. The focal or diffuse nature of the cartilage injury (pattern) is one of the main features, which guides treatment options likely to be effective.
Inflammatory Knee Arthritis (Cartilage Injury)
Inflammatory arthritis is very different than the non-inflammatory type. The cartilage damage is secondary not to repetitive stress or time or a single event trauma but is the result of a chemical process which occurs often because of an autoimmune disease. The autoimmune process causes the synovium to “attack” the cartilage surface. Instead of providing nutrition and support to the cartilage, the synovial cells secrete enzymes which essentially digest the cartilage causing it break down and resorb.
Osteoarthritis
Osteoarthritis is the most common form of knee arthritis. Most people think of osteoarthritis as the arthritis of old age. While it is true that osteoarthritis usually occurs in people over the age of 50, it may occur earlier in life. Knee osteoarthritis is considered the arthritis of older individuals because it is a “wear and tear” type of arthritis. It develops after years using the knee for seemingly normal activities.
Over time, small injuries and damage occur in the knee cartilage — so much so that the knee cartilage wears away leaving the knee bones to rub against one another. Not only is it painful to have the leg bones rub against one another, but the edges of the bone also develop bone spurs, which can cause terrible pain themselves. Unfortunately, the symptoms of arthritis get worse over time unless they are properly treated by a knee arthritis doctor.
Rheumatoid Arthritis
Rheumatoid arthritis is a disease that causes generalized inflammation. In other words, it can cause arthritis in many joints, and it can cause many symptoms throughout the body. When rheumatoid arthritis affects the knee joint, it specifically affects the synovial membranes of the knee. Synovial membranes cover many important structures in the knee including knee cartilage, tendons, bursa, and the edges of the leg bones.
Rheumatoid arthritis causes a painful swelling of the synovial membranes, which causes stiffness. Over time, the inflammation of rheumatoid arthritis can also lead to knee cartilage injuries and arthritis that affects the entire knee joint.
Posttraumatic Arthritis
Posttraumatic arthritis is a specific form of arthritis caused by injury. The key cause of posttraumatic arthritis is that the trauma to the knee disrupts the normal anatomy. For example, consider someone who was tackle in football and suffered a ruptured knee meniscus. If the meniscus does not heal properly, it can lead to arthritis.
Symptoms of Arthritis of the Knee
Virtually everyone with knee arthritis experiences pain in the affected knee. In times when the knee joint is particularly inflamed, knee arthritis patients may notice swelling and redness in the joint. In fact, pain and swelling may be at their worst when people wake up in the morning or after resting for a long period.
People who suffer from arthritis also certainly notice increased pain after strenuous exercise involving the knee joint. Less common symptoms of arthritis of the knee include the knee “giving out” (i.e. a “trick” knee) or increased pain just before a rainy weather front arrives.
Nonsurgical Knee Arthritis Treatments
Nonsurgical knee arthritis treatments vary depending on the severity of knee arthritis symptoms. The most basic knee arthritis treatments include common sense actions such as avoiding activities that tend to irritate the knee and trading activities that put a lot of force on the knee joint, like jogging, for activities that put fewer stresses on the knee joint, like swimming.
Another knee arthritis treatment that is successful for mild to moderate pain are over-the-counter pain relievers. Some people find relief from using bandages or hot or cold compresses as well. If you live in New York City, Staten Island, or Jersey City, your local knee arthritis doctor can help find the nonsurgical knee arthritis treatments that are right for you. Speaking with a local knee arthritis doctor is especially important if you have rheumatoid arthritis, since this form of arthritis can be treated with specific disease-modifying drugs. Some more common treatments are as follows:
- NSAIDS
- Physical Therapy
- Weight Loss
- Nutritional Supplements
- Corticosteroid Injectionv
- Hyaluronic Acid Injection
- Plasma Injection- Platelet Rich
- Amniotic Membrane Injection
Your knee arthritis doctor can also refer you to physical therapists and occupational therapists who can create a regimen of targeted exercises and offer assistive devices to help you improve symptoms and get around more easily.
Surgical Knee Arthritis Treatments
If nonsurgical knee arthritis treatments fail to provide relief, surgical options are available. Anyone in the local area contemplating knee surgery for arthritis should speak with a knee arthritis doctor in New York City, Staten Island, or Jersey City to discuss these options. With advanced cartilage loss and a failure of non-surgical interventions, reconstructive surgery becomes the most efficient and effective treatment option. Reconstructive treatment options for advanced cartilage loss include partial knee or total knee replacement depending on the pattern of cartilage loss.
Patellafemoral Osteoarthritis, Medial Compartment Osteoarthritis, and Lateral Compartment Osteoarthritis can affect their respective compartments alone in the very same way that other compartments of the knee are ffected. Tricompartmental osteoarthritis can affect the medial weight and lateral weight-bearing compartment along with the patellafemoral compartment.
Treatment is chosen depending on a variety of factors including the severity of the cartilage loss, level of symptoms and magnitude of disability, success or failure of previous treatments, associated injuries as well as other medical problems that may be a contraindication to oral medications, age, etc. Effective treatments include bracing and physical therapy, NSAIDS, hyaluronic acid injection, amniofix injection.
In cases of failed non-surgical treatment and/or advanced cartilage loss surface reconstruction, joint resurfacing or partial knee replacement are effective long-term solutions. There are a variety of implant systems that are well designed to reconstruct the patellafemoral surface, the medial compartment, and the lateral compartment with minimal preparation, (removal of bone) achieving restoration of normal compartmental architecture and kinematics.
There are different degrees of surgical knee arthritis treatments and repairs.
Chondroplasty
Chondroplasty is a procedure performed arthroscopically. The goal of the procedure is to reduce the ‘dead load’ of damaged non-functioning cartilage in the joint as well as creating surface stability by removing unstable surface segments.This technique is done by using a variety of surgical instruments (motorized shaver, curette, biters) in addition to an environment of saline flowing through the knee at a high and continuous rate (usually not less then 6 liters/procedure). At the completion of the procedure the cartilage surfaces should be free of any unstable segments and any loose floating cartilage removed from the joint.
Subchondroplasty
These factors are believed to be ‘irritants’ and ‘inflammatory stimulants. Thereby, removing these elements reduces the inflammatory response and reduces symptoms. There is also evidence to suggest that removing damaged cartilage helps to stabilize the bordering non-damaged cartilage and thereby would theoretically slow down the progression of the overall process satisfying what we have designated the ‘time-shift’ of disease process.
Microfracture
This method of cartilage repair is classified as a ‘marrow stimulation technique’. This procedure works best in the setting of a traumatic defect of a relatively small size (1-2 cm) and contained with healthy shoulder of cartilage bordering the lesion. The procedure is done arthroscopically and first involves cleaning the base of the lesion to removed the layer of calcified cartilage in addition to creating sharp smooth borders. Next the subchondral bone is penetrated creating multiple small channels which communicate with the bone marrow underneath.
The preference at iOrtho is to perform this step with a high speed drill and narrow diameter bit (1-2mm depending in the lesion size). Once the channels are created the mesenchymal stem cells which exist in the marrow of the bone will migrate onto the surface of the lesion and take residence.
The will then take cues from the environment and begin to perform the functions of a chondrocyte creating an extracellular matrix and filling up the defect. The cartilage that develops under these circumstances is ‘fibrocartilage’ as opposed to ‘hyaline cartilage’ on the basis of its histology and reduced amount of type 2 cartilage in favor of type 1.
This material, although it has similar mechanical properties to hyaline cartilage, is not identical and the clinical outcome studies suggest deterioration of results over time with a seemingly steeper drop off after 5 years.
Biocartilage Grafting
This method of cartilage repair includes all of the elements of microfracture with the addition of a processed cartilage allograft into the defect. The addition of the cartilage allograft into the defect has the marketed benefit of providing an existing tissue scaffold of type 2 cartilage in addition to signaling the mesenchymal stem cells by nature of containing proteoglycans and cartilage elements which serve to signal the stem cell to become more’ chondrocyte like’.
As a result the product they generate becomes more similar to normal hyaline cartilage with a greater amount of type 2 collagen compared to that found in the cartilage regenerate of microfracture alone.
Autologous Cartilage Implantation
This method of cartilage repair is best for a younger knee with a large lesion either as a primary intervention or in the context of a failed microfracture type procedure.
The technique involves harvesting a sample of cartilage from the knee taking it from an area which is non-articulating. The cartilage is sent to a specialized lab that expands the chondrocyte population and returns the expanded chondrocyte population in a refrigerated test tube on the day of the procedure. The cartilage grafting is then performed as an open procedure.
The lesion is prepared in a fashion very similar to what is described for mocrofracture with the additional step of suturing a soft tissue flap over the defect. The material used for this can be taken from the patient as an autograft or an acellular collagen scaffold can be used.
Once the defect is covered with the soft tissue and the edges are sealed with a fibrin glue the cartilage defect has been converted into a three dimensional water impermeable space. The last step is to inject the refrigerated chondrocytes into the prepared space.
The chondrocytes are held in the space by the preparation where they will take residence and create a cartilage regenerate tissue. The marketed benefit of this procedure is to create cartilage regenerate which is more similar to hyaline cartilage in terms of its histology, composition and mechanical properties. There area also clinical outcome studies also which seem to suggest that the durability of the outcomes surpass that which is typically achieved with alternative cartilage repair techniques (i.e. marrow stimulation techniques).
Osteochondral Allograft or Autorgraft
This method of cartilage repair is best for small to medium size defects (1-2cm or large defects). The technique involves harvesting a core of cartilage with its underlying bone (circular cylinder) and transferring to to an area of cartilage deficiency by removing an identically sized cylinder of damaged cartilage and bone.
It has been described as similar to a hair transplant when done as an autograft procedure. This procedure can also be done as single large graft for very large lesions with the use of a fresh frozen allograft. This procedure has the benefit of transferring hyaline cartilage which distinguishes it from all the other cartilage repair techniques. The downside is the removal and/or transfer of relatively large portions of bone which makes it a more invasive procedure then the others listed.
Resurfacing Implants/ Partial Knee Replacement
Knee cartilage damage and arthritis often develop in a pattern of deficiency which does not affect the entire joint. The knee is composed of three compartments, two weight bearing (medial and lateral) and one non-weight bearing (patellafemoral). A common pattern of cartilage damage is a single compartment (unicompartmental) or in two compartments (bicompartmental). Often under these circumstances and if other conditions are met the cartilage damage can be addressed with implants that replace only the affected compartments- unicompartmental or bicompartmental arthroplasty. The benefit of this procedure over cartilage repair is that it does not rely on a biologic healing process to restore a healthy stable surface to the joint. The knee can be immediately weight bearing and there is a much lower risk for failure of the procedure with the result being ongoing knee pain and disability.
The benefit over total knee replacement is that the procedure is less invasive with a shorter recovery time, but also and more importantly, the kinematics of the knee is not changed. This means that the knee following maturity will feel and will move the way the knee naturally moves which makes it for many people a more satisfactory procedure with the ability to return to more sophisticated physical activities. These implants are durable and have documented survivability of over 95% at 10 years which have a variety of manufacturers and systems designed for this type of procedure.
Total Knee Replacement
Knee cartilage damage and arthritis that affect the entire joint not sparing any compartments is best treated with a total knee replacement. Other circumstances which can create relative or absolute contraindications to performing a resurfacing implant may also be managed with a total knee replacement.
A total knee replacement is a procedure where the entire joint including all three compartments is resurfaced with a mono-block distal femoral and tibial implants made of metal with a modular tibial insert made of polyethylene and a patella button also made of polyethylene.
The benefit of the total knee is that addresses diffuse arthritis very effectively and can manage skeletal deformity and joint instability. When properly indicated the procedure typically registers very high satisfaction scores with knees that have little to no pain and substantially improved physical activity scores. The other benefit of a total knee replacement is that they are durable procedures with longevity rates that may approach 3 decades.